
The concept behind the federal No Surprises Act (NSA) is noble: protect patients from unexpected bills. This is a cause patients, providers, and payers collectively support. All three parties want positive patient experiences. However, this well-intentioned legislation placed impactful administrative and financial burdens on emergency medicine providers as provider reimbursement has been shrinking for years and health plan profits soar.
The NSA makes it more complex and costly than ever for providers to assure billing compliance and appropriate reimbursement. As emergency medicine group margins thin, costs rise, and reimbursement declines, it is crucial that emergency medicine groups and their revenue cycle management partners understand and address the NSA’s fiscal impact.
In this post, we unpack the fundamental ways the NSA has altered ED revenue cycle management and what your group can do to minimize its impact on your bottom line.
Why Emergency Medicine Providers are Concerned about NSA
Leading industry organizations like the American College of Emergency Physicians (ACEP) and the Emergency Department Practice Management Association (EDPMA) as well as the American Medical Association (AMA) and American Hospital Association (AHA) are strong proponents of the original goals of the NSA: protecting patients from unanticipated medical bills and keeping patients out of medical billing disputes between payers and providers. In fact, AMA and AHA were instrumental in the passing of the NSA. However, groups like the AMA and AHA and the American College of Emergency Physicians (ACEP) have filed lawsuits regarding the implementation of the NSA. And, as we write this post, at least 6 active provider lawsuits aim to bring the law’s limitations to light.
The industry-wide goal to protect patients has not changed. It is the implementation of the NSA rather than its intent that concerns providers and industry organizations. The collective concern is that the NSA will ultimately harm patients. The primary point of contention is the NSA’s Independent Dispute Resolution (IDR) process. It was intended to facilitate fair interactions between payers and providers and keep patients out of billing disputes. However, the actual result has been the prioritization of Qualified Payment Amounts/ median INN rates set by insurance companies. In short, insurance companies are paying less because IDR arbiters are required to prioritize the median INN rate they set.
Unintentionally, this disproportionately benefits commercial health insurance companies, discourages meaningful contract negotiations, shrinks provider networks, and creates unsustainable compensation for some provider practices. The overall concern is that this will ultimately make it more difficult for patients to get affordable in-network emergency care, especially in smaller or rural communities.
The Impact of NSA on Emergency Department Revenue Cycle
On top of more general NSA-related worries over patient care access and lack of payer accountability and transparency, emergency medicine providers face two additional revenue-cycle-related NSA concerns: reduced revenue and increased expenses.
Overall, the NSA documents a clear process for handling out-of-network payments. ACEP created a helpful graphic illustrating what the NSA means for emergency physicians:
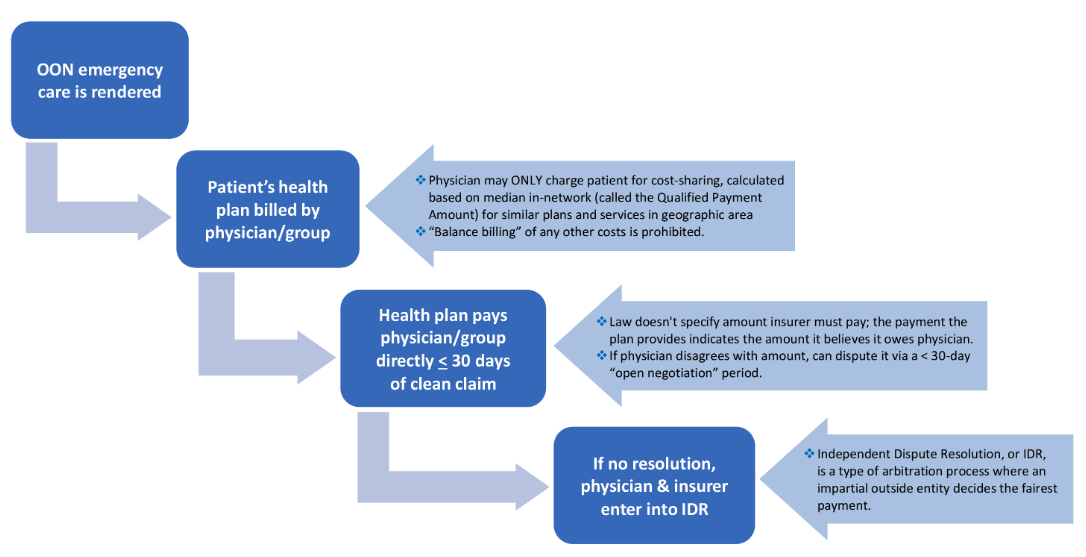
Image Source: ACEP: https://www.acep.org/federal-advocacy/no-surprises-act-overview/#:~:text=The%20No%20Surprises%20Act%3A,to%20an%20in%2Dnetwork%20facility
As mentioned, this new process impacts emergency medicine revenue cycle management at two fundamental financial levels: decreased revenue and increased expenses. Here’s a look at the two impact areas to be aware of:
Reduced Revenue
The NSA insulates patients from negotiations over out-of-network payment to providers. However, it also takes away provider leverage when negotiating payer reimbursement rate, thus reducing revenue.
NSA requirements dictate that when patients receive out-of-network emergency care, the patient’s insurer is billed by the physician group and the group can ONLY charge the patient for their cost-sharing amount. This cost-sharing amount—also called the Qualified Payment Amount (QPA) or median in-network-rate (INN)—is calculated based on the median in-network amount for similar plans and services in that geographic area. Within 30 days, insurers must pay the group indicating the total amount the plan believes it owes. If the provider disagrees with the amount, they can dispute it during a 30-day “open-negotiation” period and, if no agreement on a fair payment amount can be reached, the group can initiate the IDR process.
Since, under EMTALA, emergency medicine groups must provide care to patients regardless of their ability to pay, they have little leverage in payer negotiations (even more so now since under NSA they cannot bill historically higher out-of-network (OON) rates). Lower payments were part of the intention of the NSA, to protect patients from sometimes-egregious surprise or balance bills. However, in practice, providers seeking fair reimbursement must negotiate with payers who, in most cases, insist on paying out-of-network claims at the median INN rate for their contracted providers. The apparent goal of the health plans is to reduce the rates historically paid to OON providers and those groups with contracted rates above the plan’s mean rate.
This has led to many emergency medicine groups receiving canceled payer contracts or demands for significant cuts in contracted rates from various commercial payers. The ultimate impact is a reduction in reimbursement for emergency departments without disrupting health plan profit.
Increased Expenses
In addition to decreasing reimbursement rates, the NSA imposed additional costs on emergency medicine groups. These costs come from managing the Open Negotiation and IDR processes, in addition to other NSA-related operational processes (such as notifying patients of out-of-network status and managing increased claims denials). Managing the open negotiations period and the IDR process is complex because it has tight timelines, requirements that vary by state, and involves multiple interactions that must be tracked and evaluated.
Here is a brief overview of the details involved:
- The federal IDR process requires that commercial payers make an initial payment or issue a notice of denial within 30 days of a claim.
- Providers are then required to invoke a 30-day open negotiation process within 30 business days of the initial payment or denial
- The IDR process must be initiated within four business days of the end of the open negotiation period.
- Then, the insurer has three business days to object and the provider has four business days to submit the notice of selection of IDR entity or failure to agree.
- Both parties must submit offers to the IDR entity within 10 business days of IDR initiation.
- Within 30 days of IDR initiation, the IDR entity notifies parties of its determination, and any additional payment owed must be made within 30 days of the decision.
Just reading that “brief” overview is enough to illustrate that it is a complex task. Even with automation, these added processes can be resource intensive while offering little or no return. To combat the impact of this, it is vital that your revenue cycle management partner understand the cost of each process change and determine the ROI on each potential path designated by the NSA.
For example, your revenue cycle management partner should consider the implications of when to accept payment and when to initiate open negotiations. Additionally, they must consider what reimbursement will be acceptable to settle those negotiations and when to “pull the trigger” and initiate the IDR process. If the decision to move forward with the IDR process is made, that course involves additional costs and risks. For example, investing in a skilled negotiator for settling account-level reimbursement for services may be necessary.
In addition to understanding the risk/benefit ratio on each NSA process, your revenue cycle management partner should also have a complete picture of the impact of potentially renegotiated contracted rates that payers may demand. Projecting the revenue impact of renegotiated rates will help with overall financial planning and financial health for your group.
Mitigating the Impact of the No Surprises Act
The NSA is a well-intentioned legislation that, unfortunately, has the potential to increase management costs and reduce the revenue of well-intentioned emergency medicine groups. Besides getting involved in ACEP and EDPMA Advocacy to pursue legislative change to mitigate negative impacts on patients and providers, there are some steps emergency medicine providers can take to better protect their organization against NSA-related revenue hits.
We suggest collaborating closely with the facilities and revenue cycle partners you work with to develop a united negotiation strategy with payers. In addition to negotiating together, you can also work together to refine operational processes (such as your contracting processes and claims denial management processes) to minimize the fiscal impact of the NSA. Together you can negotiate positive managed care contracts that align your group, the facilities you serve, and the payers you contract with around improved care outcomes and efficient cash flow.
Rely on Expertise to Reduce NSA-Related Cost Increases and Revenue Reductions
A revenue cycle partner with specialized expertise in emergency medicine can help your group navigate the fiscal and operational impact of the NSA. Resolv Healthcare, a Harris Revenue Cycle Business, is that partner. Resolv provides revenue cycle management solutions for hospitals and hospital-based provider groups, ambulatory practices, laboratory practices, dental practices, and worker’s compensation and personal injury providers. Learn more about how Resolv’s 25+ years of emergency medicine revenue cycle management experience, innovative technology, and dedication to patient engagement can help improve your group’s patient experience, efficiency, and cash flow. Book your free consultation with Resolv today.
About the Author
 Richard Kleehammer CHBME
Richard Kleehammer CHBME
Rick Kleehammer currently serves as Director of Operations and Provider Advocacy for Innovative Healthcare Systems, a Resolv Healthcare company. Educated as a teacher and scientist, Rick has directed healthcare RCM operations since 2004. His experience includes leading medical coding teams, providing consulting and analytical services and leading practice and account management services. Rick is a Certified Healthcare business Management Executive through HBMA and is the current chair of the Healthcare Business Management Association (HBMA) Government Relations Committee. In addition, Rick is a subject matter expert in CMS Quality Initiatives and the evolving No Surprises Act.